



Milk fever and the dry cow diet – a hot topic for spring 2020
Milk fever was a main cause of vet visits to farms in spring 2019, writes Mary Kinston, PhD BSc
One of my favourite books, Modern Dairy Farming, originally belonging to my great-great-grandfather and printed in 1911, highlights milk fever as the most formidable of all diseases to attack dairy stock. The author, HL Puxley, cited the potential known cause at the time to be attributed to a specific microbe, but questioned this, concluding that it was a nervous condition and that the complaint was not a fever at all. It also suggests methods of prevention, such as a pound of Epsom salts given once a week, two weeks before calving, and keeping a cow with a tendency to develop the disease in lower condition prior to calving. Treatment involved distention of the udder, with one Danish practitioner developing the practise of atmospheric air being injected into the udder. Here, I have visions of a farmer using some form of bicycle pump! Thankfully, things have moved on significantly in the last 100 years – milk fever is now known as a metabolic disorder and there is greater understanding of its causes and its impact on farm. However, subclinical and clinical milk fever are still very prevalent conditions within the dairy industry, and it is the most important macro mineral disorder that affects transitioning dairy cows. While the cause of, treatment of and prevention methods are generally known, milk fever was still one of the main reasons for a spring vet call in 2019. So, we can conclude that, at farm level, its prevention and management can be somewhat sub-optimal and the cost to the dairy industry still significant. With calving upon us, the prevention and management of milk fever are, therefore, potentially hot topics for spring 2020. Vets are pivotal in the knowledge transfer required to improve farmers’ understanding of its cause and prevention of milk fever, and to effectively communicate protocols that, with a few simple but timely actions, may reduce or prevent its financial impact on the herd.
What is milk fever?
Calcium (Ca) plays a huge role in muscle function and immunity. Milk fever, or hypocalcaemia, occurs when blood Ca concentration becomes too low to support the functions of the nerve cells and the contractions of muscle tissue. Thus, milk fever is a disease characterised by reduced blood calcium levels, and clinical signs of milk fever are essentially those of a lack of muscle function. In the early stages, while this often goes unnoticed, the cow will be walking stiffly, throwing her legs to the side to retain balance, slightly blown due to lack of ruminal activity and probably constipated. With time, a classic milk fever cow is generally down, found sitting, quiet with a characteristic ‘S’ shape in her neck unable to rise. Her coat feels cold, she is either not cudding or irregularly doing so, and her temperature will be below normal. The rectum will be full of faeces and the anus often bulges. Some cows develop a fine muscle tremor, seen as shivering especially over the neck and chest. If left untreated, the muscle paralysis worsens and eventually the cow rolls over onto her side unable to sit up again. Rumen gases now can’t escape so she becomes bloated and eventually she dies.
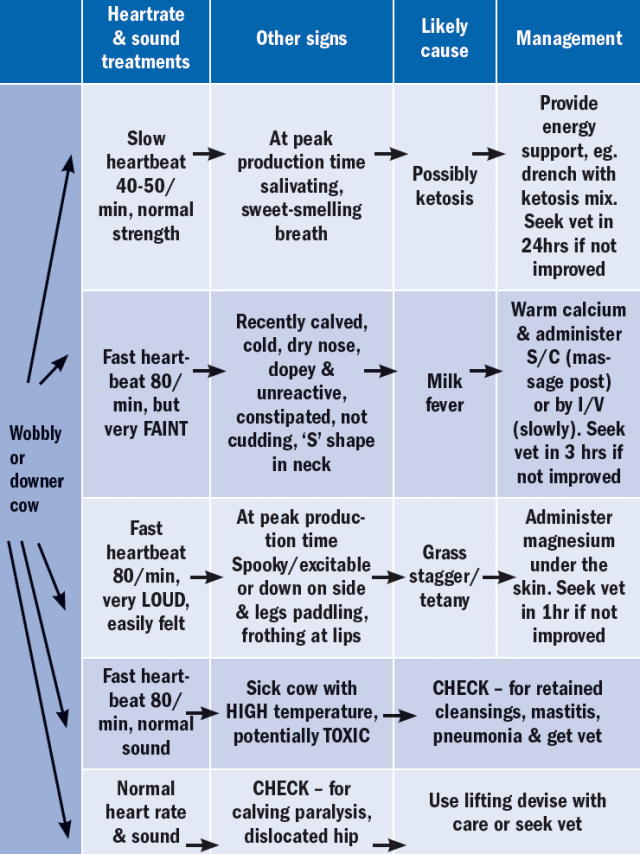
Helping farmers develop the knowledge to identify milk fever quickly can certainly be beneficial, especially where farmers are able to administer the potential treatment. However, as experience in dairying goes up and down as new people enter and older people exit the industry, there can be a role for training coupled with simple protocols and even decision trees as shown in Table 1, for a downer cow. Having such a decision tree, on farm may stop farmers presuming a downer cow has milk fever, as it’s also important to check for other conditions such as mastitis and other injuries (see Table 1).
Simply treating cows for milk fever, however, isn’t the end of the hypocalcaemia story. Ideally, milk fever should not exist in more than 2% of the herd. Clinical cases of milk fever are merely the tip of the iceberg, because for every clinical case on a farm, there can be up to 10 sub-clinical cases that are undiagnosed – though often the range is between 4-6%. Thus, for a farm with 100 cows, having two milk fever cases would indicate that there is an additional eight to 12 cases of undiagnosed, subclinical hypocalcaemia, although this could be as high as 20 cases. In addition, any of the cows that have suffered hypocalcaemia (clinical or subclinical) in the past, are more likely to be affected in future calving seasons, and to add insult to injury, both subclinical and clinical hypocalcaemia cause a cascade of other problems which can be seen on farm in the form of:
• Slow calvings
• Difficult calvings
• Retained placenta/cleanings
• Mastitis
• Displaced abomasum
• Fatty liver syndrome
• Ketosis
• Reduced milk yield (up to 1000L per cow)
• Uterine infections
• Secondary injuries to bones, nerves or muscles
• Reduced fertility from increased days to first oestrus, service and conception
It is, therefore, no surprise that studies have shown that the annual cost of sub-clinical milk fever can be greater than €6,000 in a 100-cow herd.
Prevention
Adequate status of Ca in the blood is in the range of 2-3mmol/l. This is maintained by contributions from the intestines (dietary Ca absorbed) and bones (where 99% body Ca is stored) against the losses of Ca in urine, faeces and milk. These losses significantly increase after calving due to the Ca required for milk production, with milk fever most common in the first few days of lactation, when Ca demand exceeds the body’s ability to mobilise its calcium reserves. For example, a 500kg cow can put 30g Ca into 25kg of milk every day.
Most cows manage the transition into lactation by mobilising sufficient skeletal Ca to meet the increase in Ca demand, as a newly calved cow cannot absorb enough dietary Ca to compensate for high milk production. However, cows with an inappropriate diet, hormonal imbalance or poor condition may lose more Ca than they can replace. Subclinical hypocalcaemia is seen at blood concentrations of 1.4-2mmol Ca/L. Clinical signs are usually observed 48 hours after calving – with cows exhibiting hypersensitivity, excitability, muscular twitching, weakness and rumen stagnation – and associated with blood concentration of <1mmol/L. A cow with milk fever should be propped up, kept warm and injected slowly subcutaneously or intravenously with warmed 8-14g of Ca (as calcium borogluconate). Calcium should be given at body temperature to aid absorption. When a farmer is experiencing cases of milk fever, screening of blood-calcium levels in recently calved cows can be a useful tool for assessing dietary calcium management, and can be especially useful on farms that are just experiencing high levels of a range of diseases such as mastitis, left displaced abomasums (LDAs), and endometritis post-calving.
Manipulation of the dry-cow diet is the basis for any prevention plan when it comes to milk fever. In order to implement a successful control plan, it’s vital to get a silage analysis with a full mineral profile. To prevent milk fever, before calving, dry cows should receive a diet that will ploy the metabolism into a Ca-deficient state. This will activate the parathyroid hormone vitamin D system, which acts on the bones to stimulate the release of Ca into the blood and accelerates conversion of vitamin D precursor to an active form to stimulate absorption of Ca from the diet. So, ideally farmers will feed a diet of low Ca intake 10-14 days before calving of 15-20g Ca/cow/day. Maize silage or whole crop can be useful if farmers have it as it contains less than 2g Ca/kgDM. In comparison, grass silage contains around 4.5g Ca/kgDM with intakes of 10-12kgDM/cow/day providing a higher-than-desired 45-54g Ca/cow/day. Farmers must also watch feeding silage with high clover content as grass-clover swards can contain up to 17g/kgDM. Other supplements like citrus pulp, which contains around 18g Ca/kgDM is also very high and, again, increases the risk. However, post-calving, increasing the intake of Ca to restore skeletal Ca reserves can see grass-clover swards or high Ca supplements play a beneficial role. It may also be advisable to recommend calcium supplements post calving in the form of boluses, drenches, etc. to over-conditioned cows or at-risk cows eg. twin births, previous milk-fever incidence, etc.
If we, once again, consider the dry cow, effective regulation of Ca also relies on an adequate magnesium (Mg) status as it stimulates the mobilisation of Ca from the bone. It’s also important in preventing grass tetany, so dry cows should be supplemented 10-15g Mg/cow/day from six weeks before calving to 12-14 weeks after calving. Supplementing with Mg sulphate or Mg chloride before calving is more likely to prevent milk fever than using Mg oxide as they have a higher biological availability. So, obviously even 100 years ago they were onto something with the Epsom salts, which is magnesium sulphate, although they can have a laxative effect. Interestingly, studies have shown that increasing dietary Mg from 0.3 to 0.4% of the cow’s total diet reduces that milk fever risk by approximately 62%. Therefore, we can assume that a cow needs to be provided with a diet of 42g Mg/day to prevent milk fever. A high specification pre-calving mineral will have a minimum of 22% magnesium and when fed at 100g/head/day will provide 22gMg/cow. Thus, the silage diet must provide the other 20g and this is why silage mineral analysis can be so important. Typical values in grass silage are 1.3g/kgDM meaning 10-12kgDM/cow are providing only 13-16gMg/cow/day. Unfortunately, maize silage at 1g/kgDM or whole-crop at 0.8g/kgDM are also no better so increasing the allocation of dry cow minerals to 120g/head/day (equalling 26gMg/cow) coupled with additional cal-mag or sweet cal-mag may be required where silage analysis suggests low Mg levels. Feeding minerals appropriately by applying them directly to silage at the feed barrier and not through the diet feeder, should be advised due to the variance in total feed intake prior to calving. Many farms have inadequate feed space and should be encouraged to split the minerals into two feeds or provide other forms such as blocks that cows can access freely.
A final consideration of the diet is to limit dietary potassium (K) during the dry and post-calving period. High K impairs the absorption of dietary Mg. In terms of silage analysis, farmers need to provide silage of less than 2% K. If we consider grazing and that spring pasture can be high in available potassium, if putting cow out to grass immediately post-calving, farmers need to avoid spreading high amounts of K fertiliser early on and be careful on paddocks with heavy high-soil K soil analysis. The aim here is to keep pasture K below 3.5g/kgDM. Ca status can also be affected by the cow’s dietary cation-anion difference (DCAD). Very high cation intake (K and sodium [Na]) can raise blood pH and impair the mobilisation of Ca from the bone. Therefore, the aim is to achieve a negative DCAD, but while large amounts of anion salts can improve DCAD they are poorly palatable and tend to reduce intake so need to be used with caution.
Final point to the incidence of milk fever is the management of body condition gain and score during the dry cow period. The aim must be to calve cows which are fit not fat with an optimal score between 3-3.5. The mob management of well-conditioned cows or late calver’s earlier on in the dry period can reduce problems at calving, while equally targeting first calver’s, thin cows and cows carrying twins for extra feeding can be also beneficial to avoid health issues.
1. Which of the following statements are true for milk fever prevention?
a Feed a diet of low Ca intake 10-14 days before calving
b Feed a diet of high Ca intake 10-14 days before calving
c Feed a diet high in Mg before calving
2. Which of the following pre-calving silages would reduce incidence of milk fever?
a Silage high in potassium (K)
b Silage with low amounts of K fertiliser
c Maize silage
d Silage with a lot of clover
3. What is the optimal Body Condition Score of cows at calving for milk fever prevention?
a BCS 3.25
b BCS 2.5
c BCS 3.75
Answers: 1:A&C; 2:B&C; 3:A.